


- 20 years of experience in treating complex Brain & Spine problems
- One of the largest single surgeon experience in MVD surgery for Trigeminal Neuralgia in India
- Microvascular Decompression (MVD) surgery center for Trigeminal Neuralgia
TRIGEMINAL NEURALGIA
Trigeminal neuralgia is a very painful condition causing severe misery and desperation in the lives of the sufferers. Micro vascular decompression surgery has the potential to cure this condition, if done in time and by an experienced neurosurgical team.
Achievements
Videos
Contact Us
If you want to set up an appointment with Dr. Jayadev Panchwagh for brain or spine surgery, or for consultation and expert second opinion, please call:
+ 91 9011333841, 7720948948
Between 9 AM to 5 PM.This would direct you to his team coordinator or secretary who will call you back.
Alternatively, you can send a mail to brainandspinesurgery60@gmail.com or brainpine66@gmail.com to schedule an appointment.
FAQs - Frequently Asked Questions
Where does the name ‘ Trigeminal Neuralgia’ come from?
There are two nerves – one on each side of the face – that carry the sensations of face and gums to brain where we can appreciate them. These are called trigeminal nerves. Sensations from the right side of the face are carried by the right trigeminal nerve. ‘Neuralgia‘ means nerve pain. So, Trigeminal Neuralgia is the combination of the two…meaning the pain in the region of trigeminal nerve, or in short, pain on one side of face and gums. Trigeminal neuralgia is usually unilateral (or one-sided).
But there are other causes of facial pain and gum pains. So, how do you diagnose trigeminal neuralgia specifically?
Trigeminal neuralgia is basically a clinical diagnosis. What it means is that doctors make the diagnosis by carefully listening to the patient’s history and description of the pain. The typical trigeminal neuralgia has following characteristics:
- it comes suddenly and lasts from seconds to many minutes
- it is in the distribution of the trigeminal nerve, on one side of the face
- it can start from upper or lower gum, teeth, nose, chin, cheek, just in front of the ear, forehead, eye, temple and spread to other parts of the face
The pain experienced in trigeminal neuralgia is very severe and is often described as:
- Sudden electric-current or shock-like pain
- Sudden piercing, sharp knife-like pain in the face
- Pricking of multiple sharp needles
- Sudden blast of hot bomb in the face
- Like somebody putting red-chilli powder on the face.
- Like a lightning striking the face.
Initially, the attack terminates in a few seconds or a few minutes, and then the person is usually pain-free till the next attack. In the advanced stage, the pain remains for a longer time, or become continuous for extended periods of time; and there is continuous low intensity pain between the attacks.
There are a few commonly seen trigger points, which when stimulated start the attack.
- Upper lip
- Ala of the nose
- Forehead just above the eye
- Just in front of the ear
- Upper or lower gum
- Just below the lower eyelid.
Touching one or more of these points, blast of cold, air hitting them, even a gentle breeze against them, brushing teeth (the toothbrush touching the gums), washing face, shaving, jaw movements while talking or chewing etc., can bring on the trigeminal neuralgia attack.
What can you tell us about the severity of trigeminal neuralgia?
This pain surpasses any other pain experienced by humans in severity. In short, it is extremely severe. Various patients have described this pain as:
“the worst pain ever experienced”
“the pain you should not wish even your enemies to have”
“death is better than this suffering”
“deadly curse”
“ pain of thousand knives piercing the face”
“ a hot chilli bomb exploding on one side of the face”
How do the relatives of the trigeminal neuralgia patient see this attack?
Often, in the initial phases, the relatives of the patient are bewildered as they see the patient hale and hearty one moment and, as the attack comes, the excruciating pain makes the patient miserable.
- the patient becomes suddenly immobile
- face contorted in severe agony
- tilts the head towards shoulder
- covers the painful side of the face with hand or cloth to avoid any blast of air
- does not talk, lest the attack should increase
- sometimes there is a loud groan and shriek-which indicates the unbearable nature of this pain
The patient slowly relaxes after the attack is over.
What are the personality changes which develop as trigeminal neuralgia progresses?
Along with the above-described acute effects, the life pattern slowly changes.
The relatives observe that:
- the patient avoids sitting in cold surroundings like air-conditioned rooms
- avoids going in windy atmospheres, avoids sitting in fast moving car especially near the window
- is reluctant to go to events needing socialisation which involves talking and eating, for the fear of having an attack
- is reluctant to brush teeth, wash face, shave or rub cosmetics on the affected face
- seems to have reduced appetite-even skips meals
- constantly feels tired and psychologically worn out
- severe depression may follow
- high doses of nerve and brain numbing medications makes him/her sleepy, loses balance while walking
- may develop suicidal tendencies
How does the disease progress?
In the initial phase the attacks are short and there is a long gap between them. Progressively the attacks tend to become longer, more severe and more frequent. There may be sudden disappearance of the attacks for a few days or months but gradually these attack ‘holidays’ also become rare and then disappear. In patients who are not treated in time, the attacks become almost continuous and the sufferer is reduced to a miserable creature begging for relief.
What is the cause of trigeminal Neuralgia Pain?
“Pressure (Pulsatile usually) on the nerve leaves a short-circuiting effect”.
-San Diego neurologist Dr. James Nelson
The trigeminal nerve is like a phone cable. As you know, a phone cable has insulation from the outside. But inside there are smaller cables tightly packed. Each individual small cable has, in turn, its own insulation and that’s why they cannot normally ‘Cross talk’ with each other. Otherwise an impulse from one cable can short circuit to the other cables.
Similarly, inside the trigeminal nerve, there are smaller nerve fibres. Each one has its own insulation preventing a ‘cross talk’ between them. The insulation is made up by a substance called the ‘myelin’.
The character of this myelin changes at and around the region where the nerve enters in to the brain.
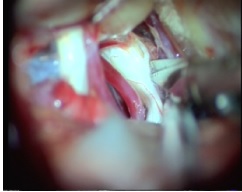
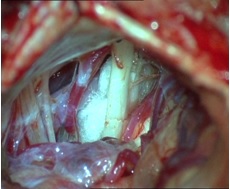
This is called the Root Entry Zone (REZ). Towards the end of the last century, it was discovered that one or more blood vessels compressing this zone (i.e. the REZ) can cause trigeminal neuralgia.
It was postulated and then proven that one or more blood vessels cause severe indentation in the REZ portion of the nerve. Months and years of continuous pulsations against this portion of the nerve damages it. This compression seems to cause damage to the myelin, which normally provides insulation to the individual nerve fibres. As a result, the nerve impulses cross-fire. A simple ‘touch’ to a portion of cheek or lip or gum gets cross fired and is perceived as sudden, severe sharp pain. This is the classical trigeminal neuralgia ‘attack”. As is well known, blood vessels in human body ‘elongate’ and harden with age. It is known as the process of ‘ectasia’. In the individuals prone to trigeminal neuralgia, the vessels originally are in close contact with the nerve. As age advances, they elongate and literally start indenting into and indeed “burying” themselves into the REZ portion of the nerve… causing damage to the myelin and starting the disease process of TN.
In some patients, during the initial days and months of the disease, the body tries to repair this damage by reforming the myelin, thus causing spontaneous disappearance of the attacks-knows as ‘pain holidays’…. only to reappear again with continued pulsatile compression or ‘hammering’ of the nerve by these blood vessels.
Generally, as the days, months and years pass, the attacks become more severe, more frequent and subsequently the pain becomes almost continuous. With the exclusion of a small proportion of trigeminal neuralgia (patients with multiple sclerosis or tumours or infarcts), the majority of the patients get trigeminal neuralgia due to the blood vessel compression.
As Dr. Peter Jennetta says, “in such patients, a careful and experienced surgeon always finds an offending vessel that is causing damage to the nerve.”
What are other reasons behind trigeminal neuralgia?
As we have seen, majority of the trigeminal neuralgia patients get pain due to severe compression by a blood vessel.
In a small proportion, tumours or cysts at the root entry zone of the nerve, causing compression and displacement of the REZ can cause trigeminal neuralgia.
However, I personally would seriously doubt that a static compression by tumour would cause trigeminal neuralgia and, after resecting the tumour, would look for an artery lodged deeply into the REZ due to the tumour pushing it into the nerve. It is also possible that the blood vessel is on the opposite side of the tumour and the tumour has pushed the nerve into the blood vessel. In one series, all the tumour related neuralgias were caused by the tumour displacing a blood vessel against the nerve. This is very major corroborative evidence that a pulsatile blood vessel compression causes trigeminal neuralgia in majority of the cases.
Multiple sclerosis, a demyelinating disease affecting the REZ or trigeminal nucleus can also cause trigeminal neuralgia in small proportion of cases. Other still less common causes could be post meningitic, brain infarcts etc.
Which investigations are carried out in the patients of trigeminal neuralgia?
The diagnosis of trigeminal neuralgia is made on the basis of a good medical history. Usually, the description of pain and the patient’s severe agony while talking, typical facial contouring and defensive facial posturing to avoid an attack, immediately give away the diagnosis. However, I always feel that along with the diagnosis of the disease, one has to acquire a fair idea about the severity of the disease.
It is very easy to assume that the patient’s pain is well controlled, if, at the moment of consultation, due to the effect of an anticonvulsant medication the patient appears free of pain. Many patients take their medication sometime before they come to see the doctor, as they rightly expect that they will have to talk a lot during the consultation. I have found time and again, that the apparently normal looking patient giving history of severe, unbearable pain attacks on the very morning.
On probing carefully the spouse, daughter or brother/sister of the patient, describe that pain attacks while the patient starts eating, I have found that the patients learn to tolerate certain amount of pain as they fear that increasing the dose of sedative anti-convulsants will make them non-functional (based on the previous experience).
What they don’t know is that there is a surgical option, having the potential to cure the disease and stop the drugs. That is the reason, why detailed history is a must.
A good quality MRI with trigeminal nerve sequences is the next step, primarily to rule out tumours. A demonstrable vessel-compressing the nerve is helpful but NOT A PREREQUISITE for surgical decision.
This is because severe vascular compression does exist, demonstrable at surgery even when MRI does not show it.
Why Micro vascular decompression?
Up until the 1980’s, most papers and textbooks listed the cause of trigeminal neuralgia as ‘unknown’ or ‘unclear’. Even today, there are different doctors advising different modalities. After trying a few of them, we strongly felt that micro vascular decompression is the right procedure (if done in time and by a surgeon and team performing these procedures routinely and successfully for a significant number of years) which has the best chance of caring for this disorder.
We have seen the happiest patients with complete disappearance of the pain after Micro-Vascular Decompression surgeries done at our trigeminal neuralgia centre in Pune, India. This personal observation and opinion is formed after 10 years of concentrated battle waged by our team against this severe pain. We have also used other modalities like radio-frequency ablation in the past and still do use it in resistant cases, as a rescue procedure. But having said this, we strongly feel that the best and the long term results are achievable by micro vascular decompression done rightly, and in time.
Why “Micro vascular Decompression ( MVD)” Centre?
After performing over 800 MVDs in the last 10 years with the help of more or less the same group of theatre assistants and anaesthesiologists at our trigeminal neuralgia centre in Pune, India, I (Dr. Jaydev Panchawagh) am personally convinced that the surgical results are significantly better if the same surgeon and the same theatre-team participate in these surgeries. We ourselves have seen remarkable betterment in the surgical outcome and quality of pain relief progressively in our own series over the last 10 years.
I also think that the nature of this surgery is very different from other neurosurgeries. Here, we are working around autonomically active nerve, which is already traumatised due to the months or years of continuous pulsatile compression by vascular structures. Also, we are working through a narrow corridor and we have to be continuously aware of the degree of tolerance or rather intolerance of the structures to maneuvering.
There are issues of preservation of draining veins, extent of mobilization of the vessels, assessing the curvature memory of the offending artery, etc. There is no single definable pathology in these cases. Every case is unique and has to be assessed on the spot during surgery. It is for these reasons that we believe that trigeminal neuralgia cases should be operated by a surgical team highly experienced in this surgery.
It was with this conviction, that we started this trigeminal neuralgia centre for Micro-Vascular Decompression surgery at Pune, India.
Incidentally, a similar technique can also be used for decompressing the facial and the glossopharyngeal nerve for treating hemi-facial spasms and glossopharyngeal neuralgia respectively. The excellence gained by the surgical team thus automatically becomes available for these disorders. Excellence in any surgery does not mean that the risks become zero, but it does mean that the risks are significantly reduced and the results are better.
Formation of a centre of excellence for MVD also allows for development of excellence in the paramedical activities like patient counselling for trigeminal neuralgia, focused training of the surgical assistant, peer communication amongst the trigeminal neuralgia patients and betterment in the post-operative treatment.
The trigeminal neuralgia centre also holds periodic meetings of those who are cured and they share their experiences and post-operative course amongst themselves and other trigeminal neuralgia patients.
This also serves as excellent feed-back for the treating team and at times, improving their approach.
It is for these reasons that we have pursued this project of developing a centre of excellence in treating the trigeminal neuralgia pain, and also for conditions like hemi facial spasms and glossopharyngeal neuralgia.
This centre offers an option to the people suffering from this severe pain, and related chronic psychological trauma associated with it, a chance to get rid of this deadly pain.
Like other modalities used in treating trigeminal neuralgia, surgery also has a potential of risks involved, albeit less. The fact is that with more experience in this field and with remarkable improvements in modern surgical and anaesthetic techniques, the risks have gone down.
When the agony and misery of the disease becomes unbearable and simpler alternatives fail, the sufferer gladly accepts the potential risks and it is at this stage that MVD has a very handsome potential of giving new pain-free life to the patients.
{kind=link}
{kind=link}
{kind=link}
Testimonials
Facebook feed
Blog

Trigeminal neuralgia the worst pain of mankind that could be cured with knife
Trigeminal Neuralgia is a very painful malady and can cause severe suffering. Microvascular decompression…Read more
Trigeminal neuralgia pain attack
Trigeminal Neuralgia Pain attack: How does it appear and how is it relieved? In this video-interview,…Read more

Trigeminal Neuralgia
Dr Jaydev Panchawagh is a top neurosurgeon (brain and spine surgeon) in Pune, Maharashtra state in India….Read more