Cervical Spine surgery from the front of neck (Anterior cervical discectomy -inter body fusion)
This operation is performed to treat damaged discs of the spine of the neck which may be protruding and causing compression of one or more nerve roots or even the spinal cord. This is diagnosed based on your symptoms and MRI. Sometimes Nerve conduction studies may be necessary to be performed. General anaesthesia is frequently required to perform this operation.
The operation involves accessing the spine from the front of the neck. Once the level of spine is confirmed by X-ray before removing it, a microscope is used to complete the procedure. The damaged disc and any bone pieces (if any) which may be compressing the nerve roots and spinal cord are also removed. This empty disc space area is then replaced with either patient’s own bone or a metallic cage which maintains the normal disc height. This means that these two spine bones will become fused together and will not move or rub against each other. Occasionally, metallic implants (like a plate and screws) are used to help with making the fusion stronger.
Dr Jaydev Panchawagh writes:
What is Cervical Radiculopathy?
Pain originating in the neck and travelling down into arm and forearm and sometimes fingers is termed as cervical radiculopathy. It is similar to “Sciatica” (where the pain starts in waist and travels down the buttock, back side of thigh and calf), but occurs in the upper limb.Along with pain there could be weakness at shoulder, elbow, wrist or fingers.
If this is because of slipped disc in the neck area of the spine, it needs careful neurosurgical treatment. Many cases do settle without surgery, but if pain is severe and weakness develops surgery should not be avoided. Radiculopathy should be taken seriously if simple measures do not work.
In this case one can see a big disc pressing on the right sided nerve.
The young man (patient) had severe unrelenting pain un the shoulder and arm and forearm for more than a month. He also had weakness at elbow.
You can see the slipped disc as shown with the red arrow.

The disc was microscopically removed followed by restoration of disc height with titanium cage. Stability achieved by titanium plate and screws.
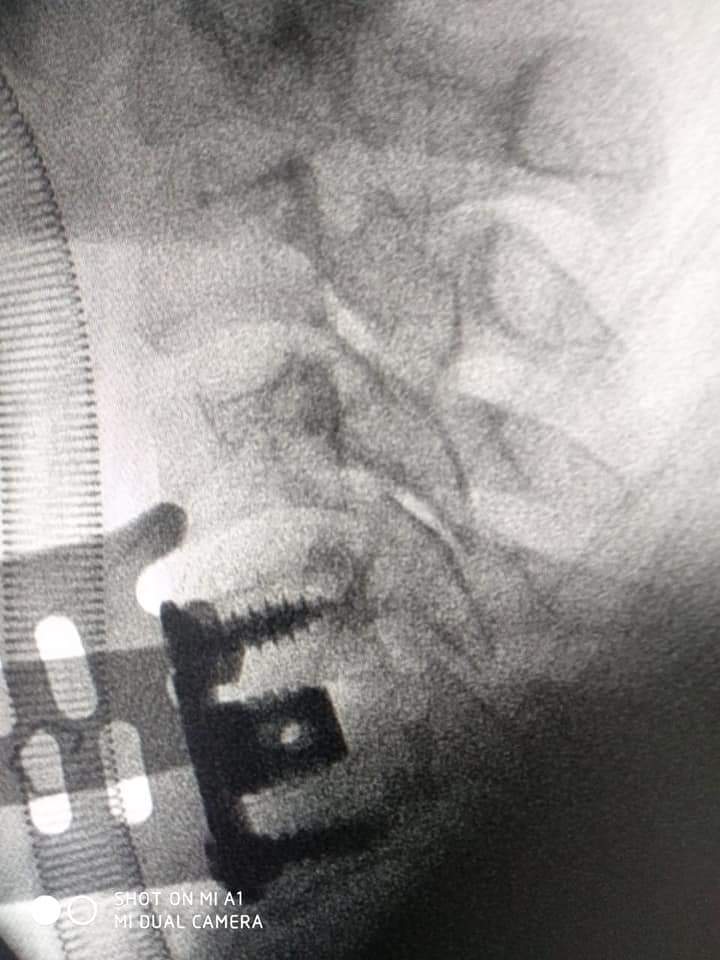
This patient was fully mobile eight hours after surgery with complete subsiding of the severe pain and return of elbow power.